
AUDITORY VERBAL THERAPY (AVT)

Anjali Sharma
(Audiologist and Speech Language Pathologist)
Introduction:
Auditory Verbal Therapy is a method for teaching deaf children to listen and speak using their hearing technology. Technology has opened up the world of opportunities for deaf and hard-of-hearing children globally.CI technology provides the modern amplification device that makes our work in AVT so much easier and allows the young deaf or hard-of-hearing child to learn faster because he now has auditory access. AVT emphasizes listening and seeks to promote the development of the Auditory cortex to facilitate learning to communicate through talking.
Definition:
AVT is defined as “ an early intervention approach for children who are deaf and hard of hearing and their families”. AVT focuses on education, guidance, advocacy, family support, and the rigorous application of techniques, strategies, conditions, and procedures that promotes optimal acquisition of spoken language through listening. (Estabrooks, 2006).
AVT provides systematic instructions to hearing-impaired children and their parents:
- Auditory – Children who are deaf learn how to listen.
- Verbal- Children who are deaf learn how to talk.
- Therapy- Parents/caregiver attends one-to-one lessons with their child and learns how to teach their children in everyday situations.
Pre-requisites of AVT:
- Early detection
- Appropriate use of hearing device
- One-on-one intervention with full parent involvement
- Absence of signs and speech reading training
- Integration with hearing peers
- On-going diagnostic therapy
Goals/ Objectives of AVT:
- The primary goals of AVT is to develop patient’s ability to recognize speech using the auditory signal and to interpret auditory experiences.
- For children to learn to listen and talk to engage in meaningful conversation, to be assimilated into regular school programs, and to have educational, social, and vocational choices throughout life.
- To develop conversation and competency in children.
Principles of AVT:
- Promote early diagnosis of hearing loss in newborns, infants, toddlers, and children, followed by immediate audiologic management and Auditory-Verbal therapy.
- Recommend immediate assessment and use of appropriate, state-of-the-art hearing technology to obtain maximum benefits of auditory stimulation.
- Guide and coach parents to help their child use hearing as the primary sensory modality in developing spoken language without the use of sign language or emphasis on lipreading.
- Guide and coach parents¹ to become the primary facilitators of their child’s listening and spoken language development through active consistent participation in individualized Auditory-Verbal therapy.
- Guide and coach parents to create environments that support listening for the acquisition of spoken language throughout the child’s daily activities.
- Guide and coach parents to help their child integrate listening and spoken language into all aspects of the child’s life.
- Guide and coach parents to use natural developmental patterns of audition, speech, language, cognition, and communication.
- Guide and coach parents to help their child self-monitor spoken language through listening.
- Administer ongoing formal and informal diagnostic assessments to develop individualized Auditory-Verbal treatment plans, to monitor progress and to evaluate the effectiveness of the plans for the child and family.
- Promote education in regular classrooms with typical hearing peers and with appropriate support services from early childhood onwards.
Significance/ Importance of AVT:
- AVT can provide opportunities to many children who are deaf or hard of hearing to learn to listen to process spoken language and to talk.
- AVT promotes early detection and diagnosis of hearing impairment consistent use of hearing device, individualized therapy and learning environment where listening and spoken language are the expected mode of communication.
- AVT helps parents to develop skills to become the primary models for speech and language development.
- AVT encourages the child to realize his auditory potential to learn spoken language communication.
- AVT is individualized and tailored to the specific needs of the child and the family.
- AVT is most effective habilitation device for children with CI because it places emphasis on audition alone.
Structure of AVT:
- The child learns to perform any task in a structured activity or game, the task must be integrated into real life situations in order to be functioned for him/her.
- Parents/ caregivers and family members are the best people to develop spoken language through listening in the home, in the natural environment.
- AVT can be taken in a hospital, clinic as private practice and in a school.
- Auditory verbal therapist takes sessions once or twice a week, for an hour with goals based on the natural patterns of child development with typical hearing.
- In each AVT sessions, the therapist provides guidance for the parents and diagnostic assessment of the child’s progress.
- AVT is considered diagnostic because it is the process of ongoing examination of the individual child’s overall progress.
Factors affecting outcomes of AVT:
- Age at diagnosis and implantation.
- Causes of hearing loss.
- Degree of hearing loss.
- Audiological management.
- Emotional state of the family.
- Child’s intelligence and development.
- Skills of the therapist.
- Family participation.
- Effectiveness of cochlear implant mapping.
Environment for AVT:
- Listening Environment:
- Speak close to child’s CI microphone.
- Speak in a quiet voice, at regular volume, raising the volume of voice can often distort speech, making it more difficult to understand.
- Minimize all background noise, turn off windows AC unit ,fan ,TV, radio.
- Use speech i.e. repetitive and rich in melody, expression and rhythm.
2. Acoustic Environment:
- Parents/ teacher/ therapist must stay within “ear shot” i.e. close to better ear within 6”-2’ or atleast within 5”.
- There should be no sequel from the child.
- Hearing device must be appropriate and well maintained 6 sounds test must be used at the beginning of the session.
The Habilitation Team
Audiologist
Pre-operatively-
- The Audiologist will determine if the child is audiologically suitable for cochlear implant. This involves determining the level of hearing loss, fitting suitable aids, assessment of benefit obtained from aids and performing other audiological investigation such as monitoring child’s middle ear infection.
- Assessment of Auditory function routinely includes behavioral assessment where a child’s responses to sound are assessed, and also objectives test such as electrophysiological assessment and OAE test should be done. Range of speech perception tests will also be conducted.
- During the pre-operative stage the Audiologist also supports the parents/ family in developing appropriate expectations and gaining a sound understanding of the technology.
Post- operatively –
- The Audiologist will conduct the switch-on of the device and the subsequent mapping sessions in the first month these are likely to be once or twice a week, then once a month for the first six months, then every three to six months or as needed.
- The Audiologist would do assessment tests such as speech perception test at regular intervals, such as every 6months for the first 2 or 3 years.
Speech and Language Therapist
Pre-operatively-
- The role of the therapist is to assess the child’s ability to hear the voice and/or other sounds whilst consistently using aids.
- Weekly goals are set for language, speech, and listening.
- The therapist would work closely with the parents to educate them about the stages of speech and language development and to counsel and inform them about realistic expectations about cochlear implant.
Post-operatively –
- After the switch-on, the therapist will continue to work with the child using the same auditory habilitation principles as were used before the operation.
- The aim is to teach the child to listen, using the sound that they receive from the cochlear implant so that they can develop effective spoken communication. The end objective would be for successful regular school integration.
Parents
- The involvement of parents is an important factor throughout the evaluation. The therapist should encourage parents to actively participate in sessions.
- Parents are taught how to create a listening environment at home where the child can learn through play, daily routines, and some planned listening activities.
- The parents are the main teachers and language models, while the therapist is teaching the parents how to interact with their child at home.
- The parents need to have knowledge and confidence to effectively apply that role in their daily lives.
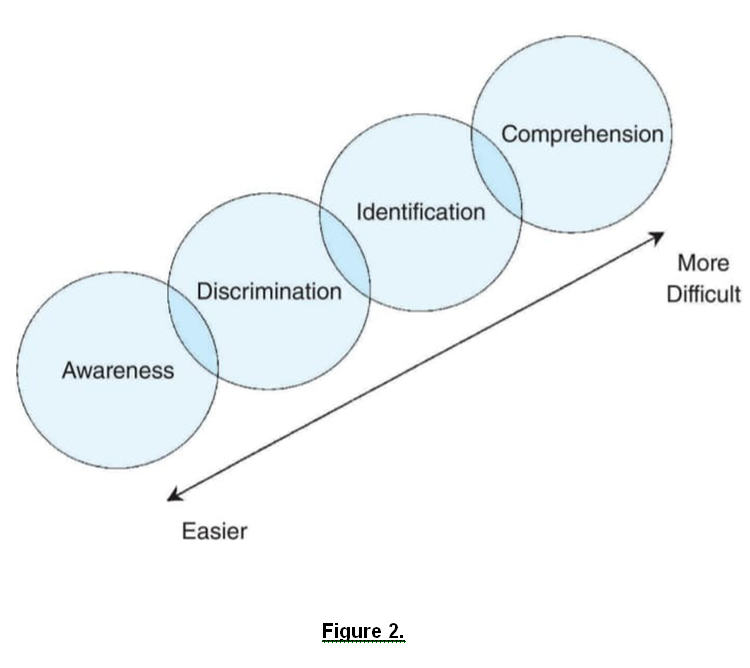
Stages of AVT
Awareness/Detection of Sound:
- It is the basic process of determining whether the sound is present or absent.
- It helps the child understand which things produce sound and which do not.
- It is also the basic steps which must be acquired before the child can be taught to associate the sound and its source.
- Awareness of sounds helps the child to remain in contact with the surrounding acoustic world.
- Ex: when father is coming home with the bike or cycle, the ringing of the bicycle and bike noise would help the child to understand to be aware.
Discrimination of sound:
- It involves perceiving the difference between sound( acoustic quality, intensity, duration etc.) Understanding that different objects producing different sounds or that the same source producing different sounds.
- Discrimination of the same vs. Different and generalization of sound into different categories.
- Ex: Discriminate between Drum and whistle sounds.
Identification:
- It involves labeling or naming what has been heard.
- The child’s can indicate the ability to identify a sound by pointing to the sound, pointing to the picture associated to the sound, pointing to the written word or sentence or even repeating what he has been heard.
- Identification of speech stimuli is related to child’s developing awareness that objects have names and these names have acoustic representation.
- Ex: Identification between the two vehicles i.e. Bus and train
.….chuk….chuk…chuk…(Train)
….vroom….vroom…vroom..(Bus)
Comprehension:
- Understanding the meaning, it depends upon the understanding skills.
- It implies that a child can acquire new information through hearing and can act appropriately on that basis and this is the pre-requisite for communication.
All Auditory learning passes through the following stages- ( Pollack,1970):
- Detection of sound
- Auditory attention
- Distance hearing
- Discrimination and auditory association
- Auditory memory span
- Auditory closure
- Auditory figure-ground
- Auditory tracking
- Listening to recording
- Auditory processing
Auditory Verbal Techniques:
- Hand cue
- Acoustic Highlighting
- Auditory Feedback
- Pausing and writing
Auditory Verbal Therapy Session:
AVT session lasts for an hour and is offered once every week at a time an date i.e. convenient to both the child and the parents. Parents are guided to understand the structure of every therapy session even though all targets are introduced through play.
The 5 Target areas addressed in every Auditory Verbal Session are-
Target | Focus |
Audition | Focus on developing listening skills. |
Language | Focus on Understanding spoken language (Receptive language). Saying or talking using specific language markers(Expressive language). |
Cognition | Focus on developing thinking skills. |
Speech | Focus on developing Suprasegmentals(duration, intensity, pitch). Segmentals(production or articulation of specific speech sounds. |
Communication | Focus on spoken language skills that facilitate social interaction. |
References:
- Foundation of Aural Rehabilitation children, adults, and their family members – 8th edition – Nancy Tye-Murray.
- Figure 1. – Developmental Areas of AVT- Estabrooks,2007.
- Figure 2.- Foundation of Aural Rehabilitation- 8th edition, Nancy Tye-Murray.
- ISHA Monograph- Auditory Verbal Therapy – by Shefali Shah
- Article on AVT- Jaspal Chowdhury, Aug 2010.
- Research outcomes on AV intervention: Is the Approach justified?- Ellen Rhoades, 22 Jan 2018.
- Auditory Habilitation for Cochlear Implant recipient: An introduction – 2005